Project: Neighbourhood-level Built Environment/Walkability and Non-Communicable Diseases in Barbados
Supervisor: Professor Ian Hambleton; Dr. Christina Howitt
Program: PhD Epidemiology (UWI Faculty of Medical Sciences and The George Alleyne Chronic Disease Research Centre)

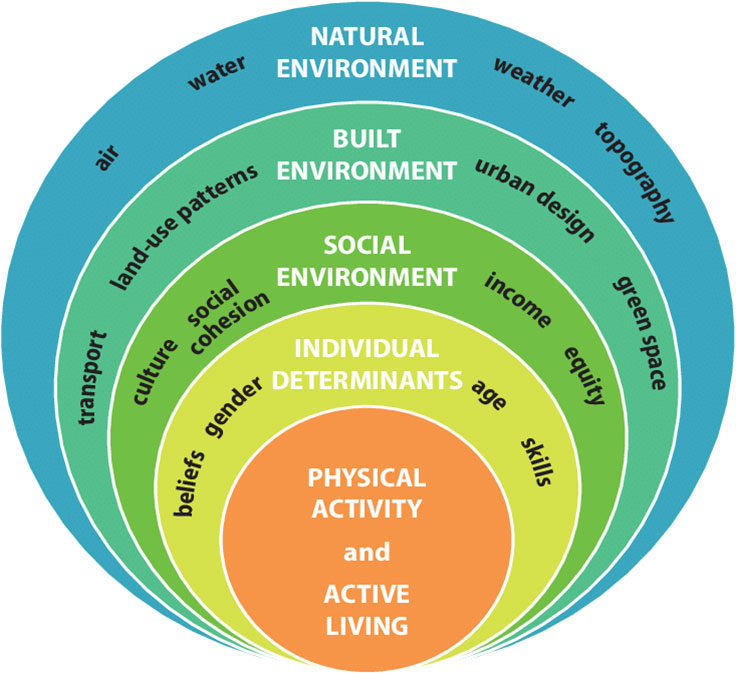
The overall aim of this project is to determine the community level walkability design; determine the presence of street-level environmental features supporting physical activity within aforementioned communities and to investigate objective and perceived individual walking behaviours of residents within these communities. This PhD research is being conducted in Barbados, with the aim of building a tool kit for expansion across other Caribbean islands. The study is designed in three phases. Phase one – Geospatial characterization of community-level walkability features (indicators of walkability, mixed land use, street connectivity, population density, and access to public transport and recreational space); Phase two – Street-level environmental features characterization (sidewalk characteristics and quality, intersections, and design characteristics) using the global Microscale Audit of Pedestrian Streetscapes tool; Phase 3 – Individual-level measurements of walking behavior using research grade activity monitors supplemented with walking diaries. This linkage of all phases with each other follows the social-ecological framework (See figure 1) in showing the interactions between the environment linking with each other to promote active living. This project spans a period of three (3) years linking with the Eastern Caribbean Health Outcomes Research Network (ECHORN) Study (Barbados Cohort).
In the Caribbean, chronic non-communicable diseases (NCDs) and their associated risk factors have increased over time to levels similar to those in developed countries such as the United States of America, Canada and some European countries , . Physical inactivity is one the four major modifiable behavioral risk factors for NCDs – cardiovascular diseases (such as heart attacks and stroke), cancers, chronic respiratory diseases (such as chronic obstructive pulmonary disease and asthma) and diabetes. Globally, there has been a rise in physical inactivity according to WHO physical activity guidelines defined as individually not meeting the weekly activity level of 150 minutes of moderate/vigorous activity , . Twenty-three (23%) of adults and 81% of adolescents (aged 11–17 years) do not meet the WHO global recommendations on physical activity for health . The Caribbean has followed similarly with Barbados reporting from the Health of the Nation study by Howitt and colleagues that objective inactivity was approximately 75% while self-reported inactivity was 47% among Barbadian adults . The WHO NCD Global Targets for 2025 has suggested that a 10% reduction in insufficient physical activity should be addressed by governments globally and the Global Action Plan for Physical Activity 2018-2030 calls for a 15% relative reduction in the global prevalence of physical inactivity in adults and in adolescents by 2030 . Despite the vast majority of CARICOM countries reporting full achievement on the implementation of ‘Public education and awareness campaign on physical activity’ , no country has reported reductions in physical activity signaling that tremendous work needs to be done to get Caribbean people moving. This will call for whole of society policies that fundamentally reshape our environments leading to active societies, environments, people and systems.
Research is key to understanding the current landscape and the priority needs. Most physical activity research evidence thus far has focused on individuals and have failed to explore the importance of community/ neighbourhood physical activity interventions. Individual-level interventions have produced mixed results with limited long-term benefit, whereas community interventions have shown promising results with longer-term benefits. There has been a gap in studying the design of communities in developing countries for the adoption of increased walking and other forms of physical activity. However, there has now been a growing body of work to understand the characteristics of the linkage between the built environment that are linked to healthy living. The United Nations in their Sustainable Development Goals called for improving the built environment in cities where it aims to achieve “universal access to safe, inclusive and accessible green and public spaces, in particular for women, children, older person and person with disabilities”. The built environment refers to man-made features or facilities that can be viewed collectively viewed as the environment whereby people live, work and socialize. Neighbourhoods contain physical and social features that influence individual health behaviours. Thus, there is a need to examine the design of these neighbourhoods from two (2) perspectives: community and street level. Community features refer to population levels within residential areas, mixed land use and street connectivity. Of particular interest in regard to community design is that of walkability which refers to environmental features that encourage walking or biking for transportation to a specific destination. On the other hand, street-level features refer to sidewalk quality, destinations availability, aesthetics and traffic calming features.
Characterizing neighbourhoods can help us gain a better understanding how to design community level interventions to aid in increasing physical activity among residents over a prolonged period of time. This type of neighbourhood characterization and linkage with individual-level data within the Caribbean is a novel multidisciplinary approach to understanding the drivers of NCD burden in the Caribbean. Potential policy implications emerging from this work can lead to improvement of the pedestrian design and inclusion of cycle paths in all communities to allow improved levels of outdoor physical activity, more active communities and ultimately contributing to reduced NCD burden.
Table 1: Showing PhD project breakdown
Figure 1: The Socio-Ecological Model